Innovation Summary
 Impaired child development is frequently rooted in inequality and poverty, leading to exposure to multiple and accumulating environmental (physical, natural, behavioural, social) and pathophysiological risks. This project links a previously validated, highly effective and culturally adapted early child stimulation intervention with an integrated, home-based environmental intervention package (IHIP). The intervention focuses on early child psychomotor stimulation and fosters age-adapted mother-child interaction by providing improved indoor air quality and indoor kitchen access to running water with a hand hygiene intervention. This integration will strengthen two critical foundations for healthy child development: i) improve parent-child relationships through responsive and stable caregiving and ii) create safe and supportive physical environments through the reduction of multiple environmental risks where children can thrive, play and develop to their cognitive potential.
Impaired child development is frequently rooted in inequality and poverty, leading to exposure to multiple and accumulating environmental (physical, natural, behavioural, social) and pathophysiological risks. This project links a previously validated, highly effective and culturally adapted early child stimulation intervention with an integrated, home-based environmental intervention package (IHIP). The intervention focuses on early child psychomotor stimulation and fosters age-adapted mother-child interaction by providing improved indoor air quality and indoor kitchen access to running water with a hand hygiene intervention. This integration will strengthen two critical foundations for healthy child development: i) improve parent-child relationships through responsive and stable caregiving and ii) create safe and supportive physical environments through the reduction of multiple environmental risks where children can thrive, play and develop to their cognitive potential.
Gallery






Impact
Expected impact:
- 160 children will receive the ECD intervention and 800 family members will use the integrated home-environmental interventions improving household air-, drinking water quality, and kitchen hygiene.
- 60% of the children <3 years will perform above the average when assessed using nationally defined development indicators.
Children learn as they play. More importantly in play children learn how to learn.
-- Fred Donaldosn, Author of Original Play®
Innovation
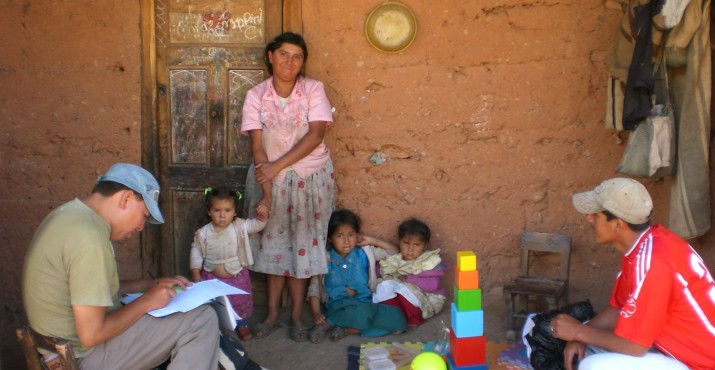
Early child development approaches need to be adapted to local contexts [1]. In combination with other, home-environmental interventions, supporting ECD may provide a cost-effective strategy to address at-risk children and impact their success and productivity through adulthood [2-4]. Our project adopts such a strategy by addressing early child development needs in concert with environmental health risks like indoor biomass fuel combustion from cooking and heating, and inadequate water, sanitation and hygiene situations. In Peru, specifically in rural contexts, addressing these exposure risks addresses the key burden of disease for children at household the level. Still, 36% (92% in rural areas) of the population primarily use solid biomass fuels for cooking and heating [5], 37% of the rural population has no or insufficient access to piped water to the home, and only 55% have access to improved sanitation [6-8].
To address these existing risk factors, this project embeds the intervention package comprising an early child psychomotor stimulation and clean cooking, drinking water and hygiene intervention into the operational plans for national development programmes. This work has been prepared by earlier research in which the ECD component of the WawaWasi National Programme was adapted for application in poor rural Andean homes (2008-10) and is now taken up by the new national child welfare programme CUNA MAS, our key project partner in this research-for-development endeavor.
Collaboration
Funders:
- Saving Brains Partners
- OPTIMUS Foundation (Switzerland)
Key partners:
- Universidad Peruana Cayetano Heredia (Peru).
- Swiss Tropical and Public Health Institute (Switzerland).
- Pontificia Universidad Católica del Peru (Peru).
- Ministry of Health (MINSA). We will work with the Cajamarca Regional Hospital and the IV RED de Salud de San Marcos (Peru).
- Ministry of Development and Social Inclusion (MIDIS), through the National Programme CunaMas (Peru).
- Ministry of Housing, Construction and Sanitation (VIVIENDA), through the Certification SENCICO Programme (Peru)
Implementation
Expected drivers:
- Working in close relationship with the Ministries and generating scientific evidence on programme effectiveness to generate a system-based, promising mechanism to enhance uptake of sustainable interventions
- Providing scientific evidence on the importance of early child stimulation and safe physical home environments to generate increased political support and lobbying for district health funds, thereby assuring financial sustainability at the outreach
- Based on the community-engaging and empowering processes used in our previous work, we expect high user-satisfaction and compliance with the different environmental intervention components (e.g. 80% are still using the stoves and sinks after six years of implementing and mothers still have the child age-specific toys or had passed them on to their neighbours)
Expected Challenges:
- Though they share the goal of developing prosperity at the rural community level, programmes relevant to this project fall under both the Ministry of Development and Social Inclusion and the Ministry of Health. Maintaining a close relationship and open dialogue with both stakeholders through intensive engagement throughout the project will help mitigate this challenge. Collaboration agreements between Cayetano Heredia University and CUNA MAS National Programme and the MoH are signed.
- Multiple stakeholders are involved, and communication and logistics between actors can translate into time delays and prolonged phases for awareness and ownership creation.
- The communities in the area in the two provinces of San Marcos and Cajabamba are dispersed and situated over a wide altitude range (1800 – 3800masl). Climatic and weather conditions may impair accessibility to communities at times.
Continuation
The project is designed as a randomized program phasing in for the regional CUNA MAS rural child development program. The program will consider the findings of this evaluation when they do the roll-out into the area and region in 2017. The aim is to establish a local flagship experience for integrated development through maintaining a stakeholder exchange platform which will allow the sharing of project and provincial program actors’ experience directly with national programmes. Both funders of our integrated home-based environmental intervention approach have strong child development and education focus. The findings of the study are shared with all interested parties (e.g. through webinars).
Evaluation Methods
The 2×2 full factorial design applies the two intervention packages 1) the environmental health intervention comprising of improved cookstoves, kitchen sinks and hygiene education (IHIP) and 2) the early child development intervention (ECD), individually and in combination. This allows for assessment of the individual effect of each intervention, as well as the assessment of synergistic effects and linkages of these interventions for programme application. The fourth group will be the control group.
Primary outcomes include:
- Diarrhea morbidity in children <3 years of age: defined according to the WHO standard of at least three loose stools passed within 24 hours.
- Acute Respiratory Infection in children <3 years of age: defined as cough and fever reported by the primary caretaker or the fieldworker.
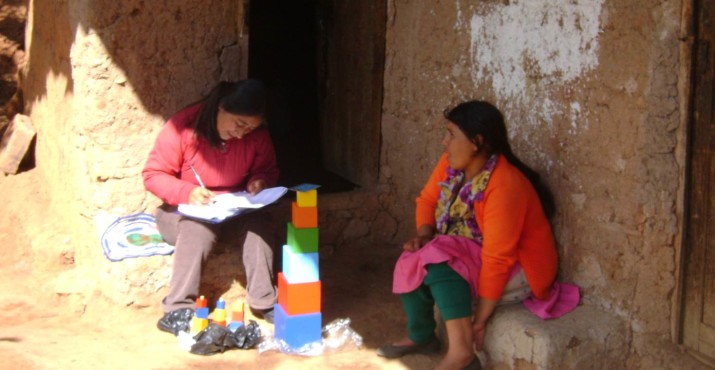
- Improvements in early child development in children <3 years of age: assessed with the nationally validated tool and defined as percentage above average for the respective age group.
Secondary outcomes include;-
- Change in socio-economic or livelihoods conditions: household assets, sustainable livelihood framework or improved home environment.
- Level of compliance of interventions
- Improved maternal child relation.
- Quality of delivered intervention: e.g. functionality of infrastructure
- Change of knowledge/attitude practices, behaviour: e.g. cookstove use and stove stacking practices, hygiene practices, water treatment, stove maintenance and repair knowledge and practice
- Change in exposure: e.g. CO plus selected PM 2.5 measures in indoor air, coli in drinking water
- Change in Nutritional Status: e.g. weight and length/height in children
Impact of Innovation
Expected Impact:
- Children in the 16 communities who receive the early child psychomotor stimulation will be more than twice as likely to score above the group mean when assessing developmental performance indicators.
- Mothers benefitting from the ECD intervention (alone or in combination with the integrated household environmental intervention) will indicate a significantly higher well-being index score than their peers in the control groups.
Cost:
- US $100,000
References
- Grantham-McGregor S, Cheung YB, Cueto S, Glewwe P, Richter L, Strupp B. Developmental potential in the first 5 years for children in developing countries. The Lancet. 2007;369(9555):60–70.
- Reynolds AJ, Temple JA. Cost-effective early childhood development programs from preschool to third grade. Annu Rev Clin Psychol. 2008;4:109–39.
- Heckman JJ, Masterov DV. The Productivity Argument for Investing in Young Children. Appl Econ Perspect Pol. 2007 Sep 21;29(3):446–93.
- Lancet T. Early child development—a winning combination. The Lancet. 2011;378(9799):1276.
- WHO / UNICEF Joint Monitoring Programme: Country Files
- Hartinger SM, Lanata CF, Gil AI, Hattendorf J, Verastegui H, Mäusezahl D. Combining interventions: improved chimney stoves, kitchen sinks and solar disinfection of drinking water and kitchen clothes to improve home hygiene in rural Peru. Field Actions Science Reports The journal of field actions [Internet]. 2012 May 31, Special Issue 6.
- Hartinger SM, Lanata CF, Hattendorf J, Gil AI, VerasteguiH, Ochoa T, Mäusezahl D, A community randomised controlled trial evaluating a home-based environmental intervention package of improved stoves, solar water disinfection and kitchen sinks in rural Peru: Rationale, trial design and baseline findings. Contemporary Clinical Trials. 2011 Nov;32(6):864–73.
- Hartinger SM, Lanata CF, Hattendorf J, Gil AI, Verastegui H, Mäusezahl D, Improving household air pollution, drinking water quality and hygiene in rural Peru: A community randomised controlled trial of an environmental, home-based intervention package. Submitted to PLoS Med
Resources
-
Research
-
Chan M. Investing in early child development: an imperative for sustainable development. Ann NY Acad Sci. 2014 Jan 1;1308(1):vii–viii.
-
Early Child Development: A Powerful Equalizer - World Health Organization
-
Hartinger SM, Lanata CF, Hattendorf J, Wolf J, Gil AI, H.Verastegui, D Mäusezahl. Impact of an early childhood development stimulation intervention on child development in rural Andean households: a community randomized controlled trial. Submitted to Lancet Global Health.
-
-
Instruments and Batteries:
-
“Lista de Cotejo” or Programme checklists: We will use the Cuna Mas internal checklist for comparison.
-
Ages and Stages Questionnaires (ASQ): Validated by CUNA MAS specialist by age group and geographical area.
-
Bayley Scales of Infant and Toddler Development (Bayley-III)
-
-
Multimedia
Similar Projects
-

CASITA
-

Chamas for Change
-

A home visiting program for pregnant youth to promote early brain development