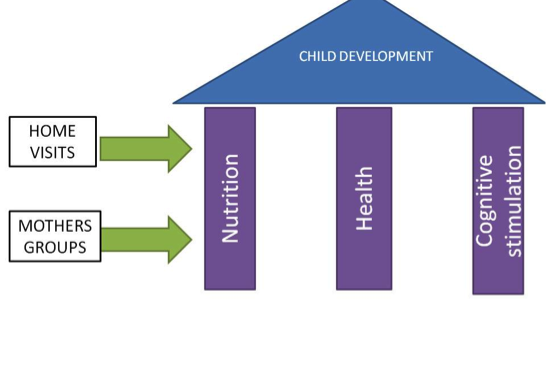
Through an existing research program (ZamCAT), nearly 40,000 pregnant women and young infants have been monitored during pregnancy and the first 42 days of child life. This existing research network will be used to demonstrate the effectiveness of an integrated community-based child development program (CCDP). The CCDP is designed to simultaneously address undernutrition, infection, and inadequate stimulation in the first two years of children’s lives. The program will use a new cadre of community based health workers — child development agents (CDAs) — to monitor and support all aspects of child development under the age of 2.
The CDAs will have three principal responsibilities:
1. Monitor nutrition and treat acute infections
CDAs will monitor children’s nutritional status on a monthly basis through home visits, and ensure immediate treatment of moderate to severe malnutrition and acute infections (malaria, diarrhea, and pneumonia) through local CHWs or public health facilities as needed.
2. Support parents to ensure children receive full health benefits
CDAs will work to ensure all children receive the full health benefits as defined in national guidelines, including exclusive breastfeeding to 6 months of age, a complete set of vaccinations, vitamin A supplementation, growth monitoring, and deworming every 6 months starting at 12 months of age.
3. Organize home-based training stimulation program
CDAs will coordinate local selected volunteer mothers to run a home-based stimulation component, where mothers meet weekly to discuss topics in ECD and learn ECD games, songs and other hands-on resources.
The curriculum for the home-based component was developed in collaboration with Save the Children Zambia and combines the Essential Package curriculum, the UNICEF CCD curriculum and other local resources. The CDAs will mentor these groups and insure their smooth functioning. The CDAs will be supported with video materials to compliment their weekly training with volunteer mothers.
Each CDA will be responsible for approximately 25 children under the age of 2 in their communities. CDAs will enroll eligible mothers and their child in the study when children are 6-12 months, and then will be responsible for the children’s health and development up to 24 months of age.
Each week, the CDA will be sent a list of mothers and children who missed scheduled services or appointments. CDAs will visit the mothers and children on this list in the respective week, and for the monthly nutrition and health follow-up as well.
CDAs have received approximately one week of training in early childhood development, plus receive ongoing quarterly refresher training. CDAs will be supported with mobile health technology to ensure continuous and efficient communication, monitoring and close implementation of service protocols. For example, the mobile device will allow CDAs to track children who are late with their vaccinations or child health visits, to communicate with local CHWs and health facility staff to ensure immediate treatment of acute health conditions, and to get feedback from referrals to the health facilities.